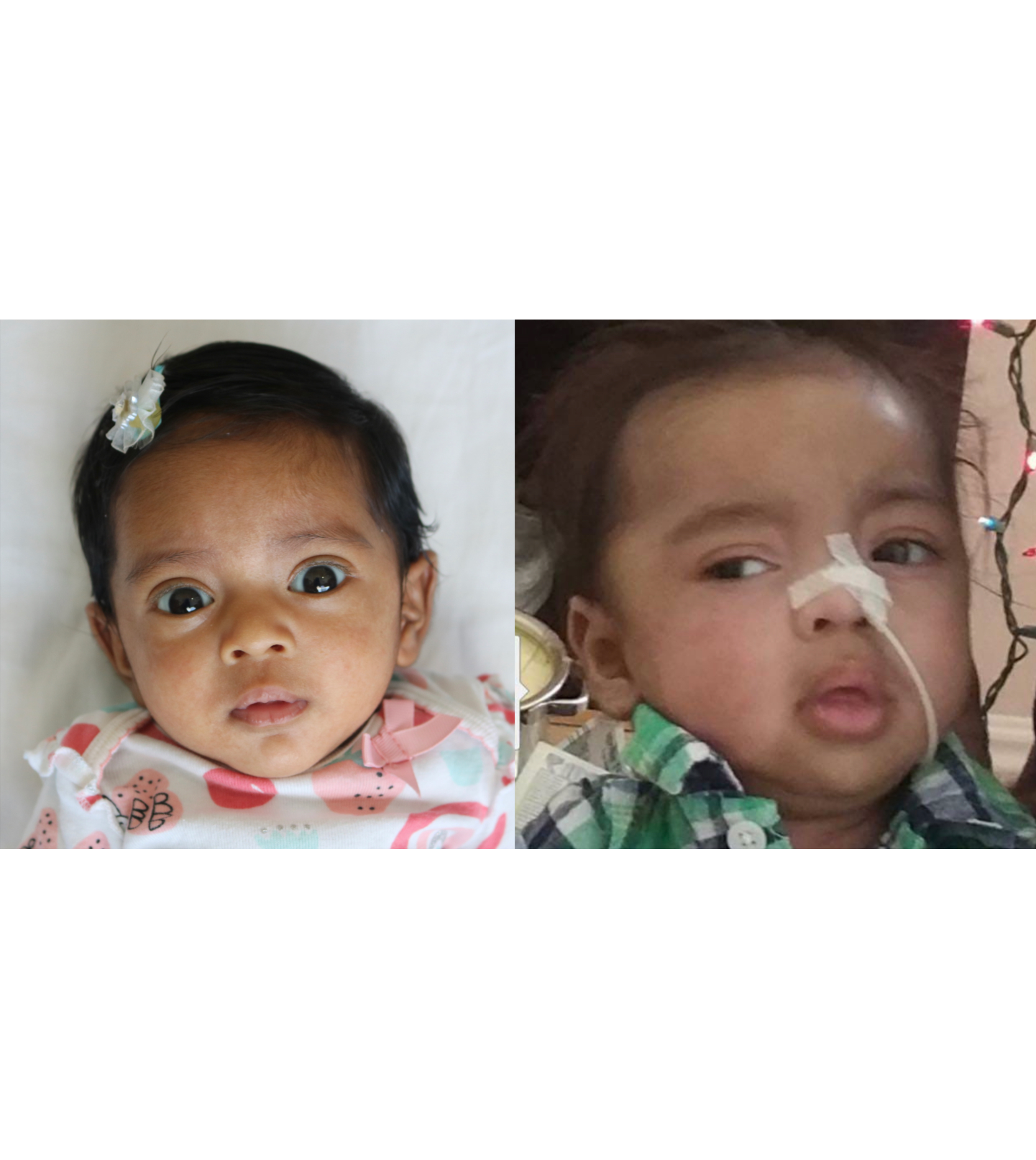
Female, age 9, with severe global developmental delay, muscle tone abnormalities (hypotonia of the trunk, hypertonia of wrists and ankles), tightened muscles and tremor of lower extremities (spasticity), brain abnormalities (cerebellar atrophy, periventricular white matter hyperdensities), and cerebral folate deficiency (decreased CSF 5-methyltetrahydrofolate concentration) caused by a change in the SPTSSA gene
Aug 20, 2020
The participant was born at term following an uncomplicated pregnancy. She was diagnosed at birth with hyperbilirubinemia. After she was discharged from the hospital, she was admitted a day later for light therapy to help control the high bilirubin levels. The participant was then discharged a day later and had to be placed in a bili-blanket for ten days. Concerns about her development first arose at around 4-6 months of age when poor head control was noticed, and she wasn’t rolling over (global developmental delay). Due to the presence of a port-wine stain birthmark on her forehead (nevus flammeus) and developmental delays, a diagnosis of Sturge-Weber syndrome was considered at this time. This was later ruled out after a MRI was conducted.
The participant was diagnosed with cerebral folate deficiency syndrome after spinal fluid was tested for metabolic conditions. Due to a diagnosis of failure to thrive and a suspected underlying metabolic disease the participant had a G-tube placed at 2 years old. The participant also began to experience recurrent vomiting with aspiration causing recurrent pneumonia. As a result, she underwent a Nissen fundoplication at age 5. This procedure decreased the frequency of her pneumonia hospitalizations, but she still had breathing difficulties. Additionally, she had a gap between her larynx and esophagus (laryngeal cleft) which has since been repaired, has difficulty swallowing (oropharyngeal dysphagia), and excessive drooling (sialorrhea) which is controlled with scopolamine patches and Botox injections in her salivary glands.
The participant has increased muscle tone (hypertonia) most significantly affecting her wrists and ankles. Her muscles are tight in her legs (spasticity) with a tremor. She did not respond to Sinemet treatment.
The participant experiences recurrent UTIs, and at age 6 had kidney stones removed (nephrolithiasis). These were presumably caused by her abnormal kidney function (renal tubular acidosis).
A metabolic condition was suspected due to intermittent metabolic acidosis and slightly elevated lactates. A brain MRI showed volume loss most significantly affecting the deep gray nuclei and cerebellum. Currently the participant is nonverbal and is unable to sit upright independently, roll over, or grab objects (global developmental delay). However, she is cognitively alert, smiles appropriately, shows affection, and tracks well with her eyes.

Clinicians and researchers believe a de novo genetic change in the following gene may be causing the participant’s symptoms.
If this participant sounds like you or someone you know, please contact us!